Institute Research Priority Plan 2024-2034
Reimagining Acute Care: Delivering better outcomes for all Canadians through research and evidence-informed decision-making
Institute Research Priority Plan 2024-2034
Cat. No. MR4-203/2025E-PDF
ISBN 978-0-660-79357-3
Land Acknowledgement
The Canadian Institutes of Health Research Institute of Circulatory and Respiratory Health (CIHR-ICRH) is hosted at the Research Institute of the McGill University Health Centre (RI-MUHC), located in Tiohtià:ke/Montréal. We respectfully acknowledge that the land on which we developed our Institute Research Priority Plan (IRPP) is situated on the traditional and unceded territory of the Kanien'kehà:ka, a place which has long served as a site of meeting and exchange among many First Nations.
As an institute with national reach, we honour all Indigenous Peoples (First Nations, Inuit and Métis), from coast to coast to coast. We acknowledge their past and ongoing contributions to society and deeply value the strength and wisdom of Indigenous knowledge systems and holistic approaches to wellness that have guided generations.
We recognize that the impacts of colonization continue to shape health outcomes and access to care. CIHR-ICRH's commitment to improving the health of all Canadians includes a responsibility to engage meaningfully with Indigenous communities. Our goal is not only to foster respectful and reciprocal relationships, but to build genuine allyship, ensuring Indigenous voices, leadership, and representation are present across all aspects of our work.
As we continue on a path towards healing, reconciliation and self-determination, we invite members of our research community to learn about and reflect upon the Indigenous Peoples whose traditional territories they reside on.
Message from the Scientific Director
Discovery is one of the most exhilarating dimensions of the human experience. Over the past century, science has evolved at an unprecedented pace, bringing us to a new era of interdisciplinary innovation. As we navigate the transition between centuries, our ability to explore uncharted ideas has expanded, empowering us to reimagine a healthier future for all Canadians.
Canada has a proud legacy of leadership in cardiovascular and respiratory research. In 1947, Dr. Wilfred Bigelow pioneered the idea of using hypothermia to enable heart surgery, an innovation that reshaped modern cardiac care. Canadian researchers have also been instrumental in key breakthroughs in pulmonary medicine, including the discovery of the gene responsible for cystic fibrosis.
Building on more than 80 years of rapid advances in cardiopulmonary science, our research community is poised to drive the next wave of transformation in public healthcare. We stand at a pivotal moment when science can directly inform patient-centred, policy-relevant, and system-wide improvements across the full continuum of care.
The Institute of Circulatory and Respiratory Health (ICRH) is proud to present its 10-Year Institute Research Priority Plan (IRPP), a bold and forward-looking blueprint to revolutionize how acute care is conceived and delivered in Canada. Rooted in scientific excellence, this plan goes beyond research funding. It reimagines care before, during, and after medical crises, harnessing the power of emerging technologies to reshape outcomes.
We invite you to join our scientific community in advancing this vision: To reduce the burden of acute disease, improve treatment outcomes, accelerate recovery, and help build a sustainable, equitable, and resilient healthcare system for all Canadians.
Ariane Marelli, MD, FRCPC, MPH, FCAHS
Scientific Director,
CIHR Institute of Circulatory and Respiratory Health
The Changing Landscape of Acute Care
From pioneer work in cardiac surgery and pulmonary medicine to contemporary discoveries in sleep science and stroke management, Canadian researchers have consistently pushed the boundaries of medical knowledge. Despite these advances, cardiovascular and chronic respiratory diseases remain among the leading causes of death in Canada, and represent the main drivers of acute care hospitalization. As our healthcare system wrestles with escalating pressures, from aging populations to workforce shortages and rising hospital costs, the time has come to reimagine how research can drive impact where it is urgently needed: acute care.
ICRH's Institute Research Priority Plan (IRPP) sets forth a transformative strategy focused on improving health outcomes, advancing discovery, and aligning science with pressing health system challenges. At its heart is an urgent conundrum: Canadians are arriving too late and staying too long in acute care. We must intervene earlier, treat more precisely, and support recovery more effectively and efficiently to improve outcomes.
This IRPP reflects a renewed vision to align research investment with the needs of our population, within an emerging national context that calls for innovation. It builds on Canada's recognizable strengths in artificial intelligence (AI), digital health infrastructure, and biotechnology, echoing the government's strategic emphasis on turning health research into a driver for economic growth.
ICRH Canada's Acute Care Strategy (CAre)
Our 2024-2034 vision is to reimagine acute care in Canada through research and evidence-informed decision-making. To support this vision, we propose CAre, a strategic framework designed to transform acute care delivery across Canada. This initiative aims to improve outcomes for Canadians living with complex conditions within ICRH's mandate areas across the lifespan. By addressing the full continuum of care (pre-acute, acute, and post-acute diseases), CAre seeks to prevent hospitalization for at-risk patients, improve outcomes of acute care medical and interventional procedures, and increase the efficiency and effectiveness of recovery for sustainable health.
This plan integrates real-world experience, robust evidence, and a bold ambition to make research matter at the point of care. It draws upon extensive engagement with researchers, clinicians, community leaders, and people with lived and living experience (PWLLE), and is informed by evidence and shared values, collaboration and partnerships. ICRH's strategy will unfold through evolving phases designed to strengthen the research ecosystem, expand collaborative capacity, and deliver measurable results in acute care.
Our aspiration is clear: Improving the current landscape of acute care for Canadians by enabling the right care to the right patient at the right time.
Who We Are
ICRH is one of the thirteen (13) Institutes of the Canadian Institutes of Health Research (CIHR).
We are guided by an Institute Advisory Board (IAB) composed of researchers, clinicians, policymakers, and people with lived and living experience. Together, we ensure that our research investments target both emerging science and the needs of Canadians, while fostering equity, innovation, and measurable impact.
Mission
To support research into causes, mechanisms, prevention, screening, diagnosis, treatment, support systems, and palliation for a wide range of conditions associated with:
- Heart
- Brain (Stroke)
- Lung
- Blood/Blood Vessels
- Sleep
- Critical Care
Values
Developed through meaningful engagement with our community and partners, our values represent the foundation of our strategic direction.
- Science Excellence: Research that is rigorous, relevant and interdisciplinary.
- Evidence-Driven Decision-Making: Data and real-world evidence to guide practice and policy.
- Discovery for Social and Economic Impact: Research that improves care and fosters innovation-driven growth.
- Patient and Family-Centred Care: Lived and living experience embedded in research design and delivery.
ICRH is committed to embracing CIHR priorities represented in the CIHR Strategic Plan 2021-2031, entitled A vision for a healthier future.
- Advance Research Excellence in all its Diversity
- Strengthen Canadian Health Research Capacity
- Accelerate the Self-Determination of Indigenous Peoples in Health Research
- Pursue Health Equity through Research
- Integrate Evidence in Health Decisions
ICRH's Vision for 2024-2034
ICRH Canada's Acute Care Strategy (CAre) - A strategic framework: Evidence for better care
ICRH's framework addresses the Acute Care Conundrum. Simply stated, patients are arriving at the hospital too late to fully benefit from timely interventions and are staying too long with a growing number of disease complications. The jump in expenditures before and after the COVID-19 pandemic, together with the reduced resilience of the healthcare system, has created a nexus for the crisis in acute care we are seeing across Canada. Most alarming, the rising cost and declining quality of our public healthcare are opening the door to increasing health inequity for Canadians.
The proposed solution is reimagining acute care through evidence-based decision-making that delivers better results for Canadians. Acute disease doesn't just appear suddenly, and it doesn't end when the crisis is over. It exists within a broader continuum of care that begins well before and lasts long after the acute event.
The Acute Care Conundrum
- Patients arriving too late and staying too long
The Result
- Escalating medical complications and acute care costs
The Proposed Solution
- Reimagining acute care in Canada: Delivering better outcomes for Canadians through research and evidence-informed decision-making
Why Our Work Matters
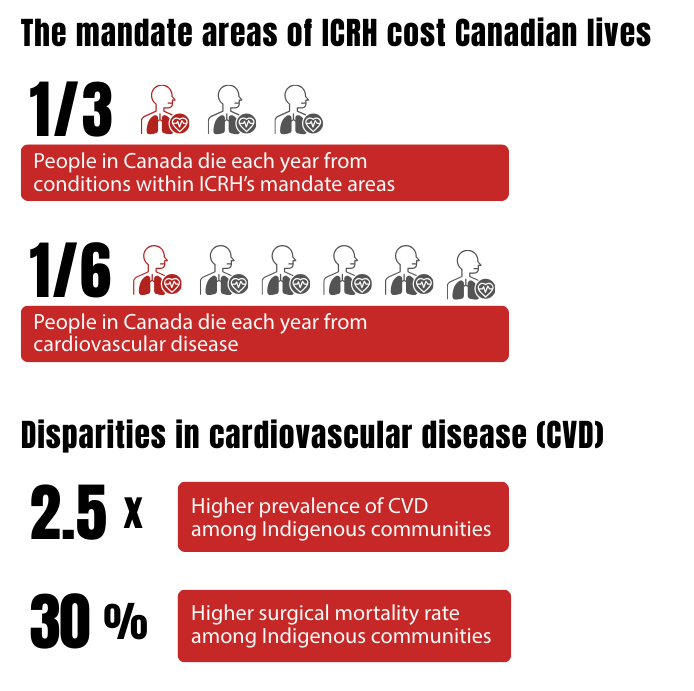
Cardiovascular, respiratory, cerebrovascular and critical care conditions are among the leading causes of death and hospitalization in Canada. They account for approximately one in three deaths, with one in six attributed specifically to cardiovascular disease.Footnote 1 These conditions are particularly prevalent in adults aged 65 and above,Footnote 2 and the burden is greater in Indigenous communities, where cardiovascular disease is 2.5 times more common and surgical mortality rates are 30% higher.Footnote 3
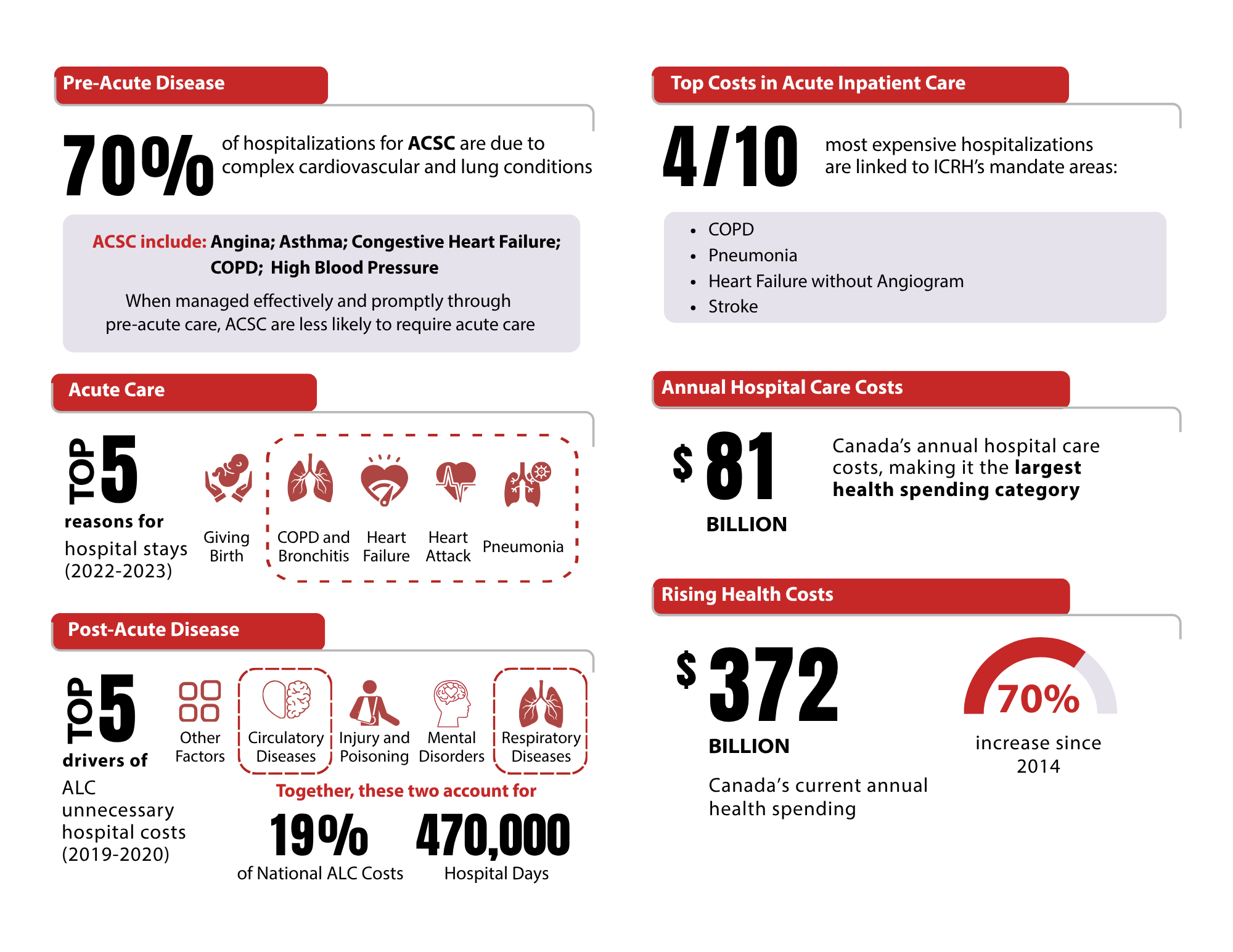
Ambulatory Care Sensitive Conditions (ACSC), including angina, asthma, congestive heart failure, chronic obstructive pulmonary disease (COPD), and high blood pressure, can be managed through timely pre-acute care.Footnote 4 Yet, about 70% of ACSC hospitalizations are still due to cardiovascular and lung conditions,Footnote 4 contributing to four of the top five reasons for hospital stays.Footnote 5 More broadly, circulatory and respiratory diseases are two of the top five drivers of costs related to Alternate Level of Care (ALC), in which patients no longer need acute care but remain in hospital, accounting for 19% of the national total ALC costs and representing 470,000 unnecessary hospital days.Footnote 6 These are not just health statistics, they are missed opportunities. Missed chances to intervene early, to connect research with bedside, and to harness innovation and digital tools to transform care delivery.
Four of the ten most expensive hospitalizations in Canada are linked to ICRH's mandate areas.Footnote 7 With hospital care representing the largest health expenditure at $81 billion annually,Footnote 8 and overall health spending rising by 70% over the past decade to $372 billion,Footnote 9 there is an urgent need for strategic investment in translational research and systems improvement. Over the past 25 years, ICRH has significantly invested in fundamental discovery and clinical science. To maximize its impact, ICRH will focus on acute care research with a multi-disciplinary and interdisciplinary approach. ICRH firmly believes that with the right investments, Canada can bridge its legacy of scientific excellence with a future of health innovation.
Key Metrics
ICRH's mission is to support research that addresses some of Canada's most pressing health challenges, including heart, lung, brain (stroke), blood, blood vessels, critical care and sleep.
Long description
The mandate areas at ICRH cost Canadian lives:
- One (1) in three (3) people in Canada die each year from conditions within ICRH's mandate areas
- One (1) in six (6) people in Canada die each year from cardiovascular disease
Disparities in cardiovascular disease (CVD):
- There is a 2.5 times higher prevalence of CVD among Indigenous communities
- There is a 30% higher surgical mortality rate among Indigenous communities
Long description
Pre-Acute Disease
- 70% of hospitalizations for ACSC are due to complex cardiovascular and lung conditions
- ACSC include: Angina, Asthma, Congestive Heart Failure, COPD, and High Blood Pressure
- When managed effectively and promptly through pre-acute care, ACSC are less likely to require acute care
Acute Care
- Top 5 reasons for hospital stays in 2022–2023:
- Giving Birth
- COPD and BronchitisFootnote *
- Heart FailureFootnote *
- Heart AttackFootnote *
- PneumoniaFootnote *
Post-Acute Disease
- The top 5 drivers of ALC unnecessary hospital costs for 2019–2020 include:
- Other Factors
- Circulatory DiseasesFootnote *
- Injury and Poisoning
- Mental Disorders
- Respiratory DiseasesFootnote *
Together, circulatory and respiratory diseases account for:
- 19% of national ALC costs
- 470,000 hospital days
Top Costs in Acute Inpatient Care
- 4 out of the 10 most expensive hospitalizations are linked to ICRH's mandate areas:
- Chronic Obstructive Pulmonary Disease (COPD)
- Pneumonia
- Heart Failure without Angiogram
- Stroke
Annual Hospital Care Costs
- $81 billion represent Canada's annual hospital care costs, making it the largest health spending category.
Rising Health Costs
- $372 billion represent Canada's current annual health spending, marking a 70% increase since 2014.
How We Developed the Strategy
ICRH's IRPP is grounded in a systematic nationwide engagement process. Throughout 2024 and into 2025, ICRH visited 22 knowledge exchange sites, conducted targeted interviews with PWLLE and provider groups, and launched a national survey to gather collective insights. These efforts were complemented by key informant interviews and a review of strategic priorities across CIHR and peer institutes.
We listened carefully to our research community, partner organizations, PWLLE, clinicians, policy leaders, and previous successful ICRH-funded research teams to understand what is needed and what is possible in the years ahead.
The Message Was Clear
To be relevant, impactful, and future-ready, research should help close the gap between discovery and care, especially in acute settings. Reducing the gestation time between discovery and implementation requires structured programs and partnerships that accelerate the transition from laboratory insight to bedside improvement.
Engagement Activities
- 11 Canadian Regions
- 22 Site Visits
- 6 IAB Feedback Sessions
- 13 Key Informant Interviews
- 266 Survey Respondents
Participants
- Research Community
- Partner Organizations
- PWLLE
- Clinicians
- Policy Leaders
Key Themes
- Data-Driven Approach: Leverage Canada's data to bridge research and care, considering diverse populations.
- Research for Care: Align research with clinical needs to inform precision care.
- Integration with Clinical Work: Support initiatives to integrate research and practice.
- Economic Impact: Advocate for investments in health innovation to drive economic value.
- Clinical AI & Digital Tools: Apply AI methods to accelerate discovery to implementation across research platforms.
- PWLLE Advocacy & EDI: Ensure PWLLE and community involvement with a focus on equity, diversity and inclusion (EDI).
Our Strategy
Improving the Care Continuum Across the Lifespan
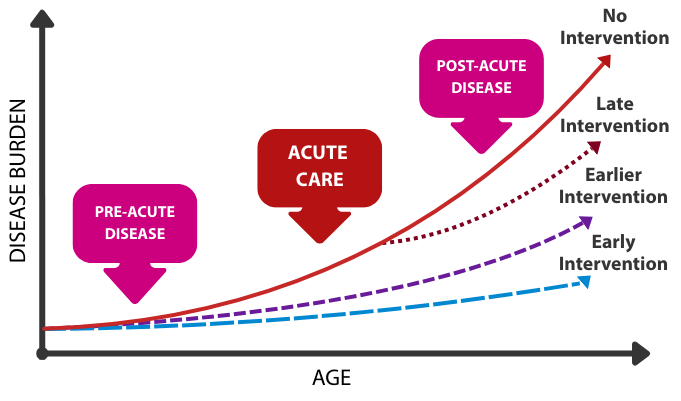
ICRH's conceptual framework spans the care continuum across the lifespan, from pre-acute and acute through to post-acute stages. This continuum provides a system-level view of how acute health events unfold, guiding the use of targeted interventions at each stage to help reduce disease burden across the lifespan. As the disease burden escalates over time, from pre-disease risk factors to acute episodes and post-acute consequences, the precise timing in medical and procedural interventions is paramount.
The figure below illustrates how earlier treatment and prevention not only reduce disease burden but also improve health trajectories. When interventions are delayed, outcomes worsen, contributing to the accumulation of multi-system disease, placing greater strain on our healthcare system. ICRH's strategy focuses on shifting from reactive care to proactive approaches, where early intervention helps reduce disease progression at every stage.
Long description
The image is a line graph with the x-axis labelled "Age" and the y-axis labelled "Disease burden." It displays four curves representing different intervention strategies over time:
- A solid red line labelled "No Intervention" shows a steep increase in disease burden with age.
- A dotted red line labelled "Late Intervention" follows a similar path but slightly lowers the burden in later stages.
- A dashed purple line labelled "Earlier Intervention" shows a more gradual increase and lower peak.
- A dashed blue line labelled "Early Intervention" maintains the lowest disease burden across all ages.
Three arrows point to specific points on the solid red line, marking stages of disease continuum:
- Pre-acute disease
- Acute care
- Post-acute disease
The graph visually emphasizes that earlier interventions lead to lower disease burden over time.
Strategic Framework
To reimagine acute care in Canada, ICRH is focusing on three interconnected priority areas across the disease continuum: pre-acute; acute and post-acute. These priorities will form the backbone of our research initiatives and partnerships with collaborators from clinical settings, academic institutions, government, and industry.
ICRH's IRPP aims to improve acute care outcomes for Canadians with cardiovascular and respiratory conditions promoting health span across the lifespan.
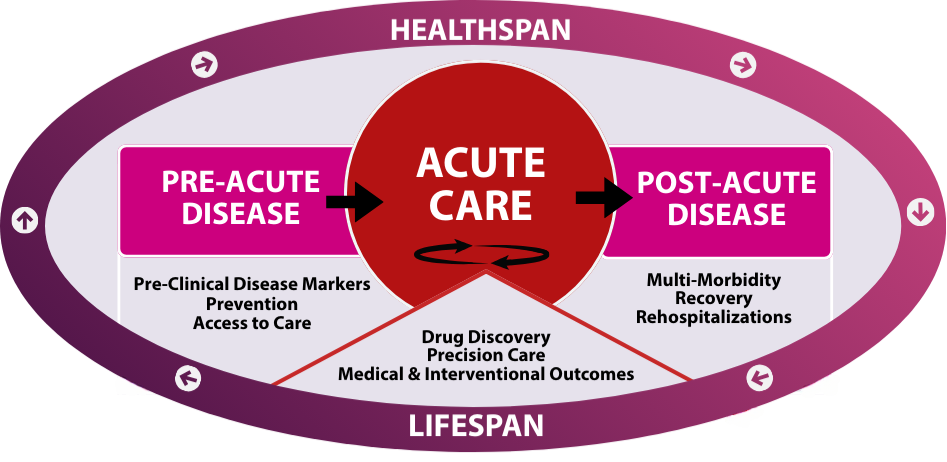
ICRH Canada's Acute Care Strategy (CAre): A strategic framework: Evidence for better Care
Long description
The graphic is structured around three main stages of disease and care:
- Pre-Acute Disease
- Pre-Clinical Disease Markers
- Prevention
- Access to care
- Acute Care
- Drug Discovery
- Precision Care
- Medical & Interventional Outcomes
- Post-Acute Disease
- Multi-Morbidity
- Recovery
- Rehospitalizations
These stages are arranged within an oval frame, with "Healthspan" labeled at the top and "Lifespan" at the bottom, suggesting a continuum of health across a person's life.
Each stage is enclosed in a separate box: Pre-Acute Disease on the left, Acute Care in the center and Post-Acute Disease on the right.
The Acute care section is highlighted with a large red circle at the centre of the oval. Beneath this circle is a triangle, symbolizing balance between the surrounding stages with a circular arrow, representing the recurring and dynamic nature of acute medical interventions.
A single directional arrow flows from the pre-acute box into the central Acute care circle, followed by another arrow extending from the Acute care circle into the post-acute box, illustrating the continuum of care from early intervention through acute treatment to recovery.
Strategic Priorities
Pre-Acute Disease
The best acute care is the one we never need. Preventing medical crises before they happen is both a health and economic imperative. Yet today, too many Canadians lack access to early care, a critical factor in preventing and delaying hospitalization. Conditions like chronic obstructive lung disease, asthma, heart failure, and hypertension account for over 70% of potentially avoidable hospital admissions.
ICRH will prioritize research on biological markers, AI models for risk stratification and preventive approaches, including social, structural and economic determinants of health, lifestyle and environmental factors. These efforts will be complemented by scalable community-based interventions that improve access to primary and subspecialty care, helping flag risk earlier and directing support toward those most in need.
Objective
- Preventing hospitalization for at-risk patients
Areas of Focus
- Pre-clinical disease markers
- Prevention
- Access to care
Measures of Success
- Novel biomarkers
- Increased understanding of mechanisms of disease
- New risk modelling approaches integrating network data & AI
- Reduction in number of avoidable hospitalizations
Acute Care
For patients experiencing an acute event such as stroke, heart attack or sepsis, the speed and quality of care can mean the difference between life and death. ICRH will invest in drug discovery, clinical trials, tools, and AI-enhanced technologies that advance the quality of acute medical and interventional procedures in a timely manner.
We will focus on improving precision care, including processes of acute care delivery for diagnoses, triage, and interventions in emergency and critical care environments. Pulling together advances in science and care for cardiovascular, respiratory, cerebrovascular, blood and sleep disorders, we will promote the management of acute disease to improve outcomes and shorten the length of stay in acute care settings.
Objective
- Improving outcomes from medical & interventional procedures
Areas of Focus
- Drug discovery
- Precision care
- Medical & interventional outcomes
Measures of Success
- Number of clinical trials
- Advances in precision care outcomes
- Development of integrated care frameworks
- Reduced hospital length of stay
Post-Acute Disease
Despite advances in acute care, the mechanisms that drive the progression from acute illness to chronic co-morbidity remain poorly understood. Our healthcare system is unprepared to receive patients where disease may be indolent but at risk of recurrence. Too many patients are discharged without adequate resources for sustainable recovery, leading to unnecessary medical complications and costly readmissions.
ICRH will support research focused on understanding the mechanisms of transformation from acute disease to complex multi-systemic diseases. We will champion implementation science and promote community-based recovery models, including primary care reintegration. ICRH will also support the development and deployment of digital tools that support continuity of care, such as remote monitoring, AI-assisted rehabilitation, and chronic care integration aimed at preventing rehospitalization.
Objective
- Enhancing sustainable & effective health recovery
Areas of Focus
- Multi-morbidity
- Recovery
- Rehospitalization prevention
Measures of Success
- Markers of transformation from acute to chronic disease
- New protocols for post-acute care disease management
- Reduced hospital readmission rates
Strategic Enablers
Transforming acute care requires more than research, it requires the right conditions to apply and scale-up research outcomes. To enable results that are patient-centred, policy relevant and impactful, ICRH will prioritize enablers across three critical domains, in collaboration with colleagues across CIHR and external partners.
- Research Infrastructure
- Health Data, Digital Tools and AI
- Learning Health System
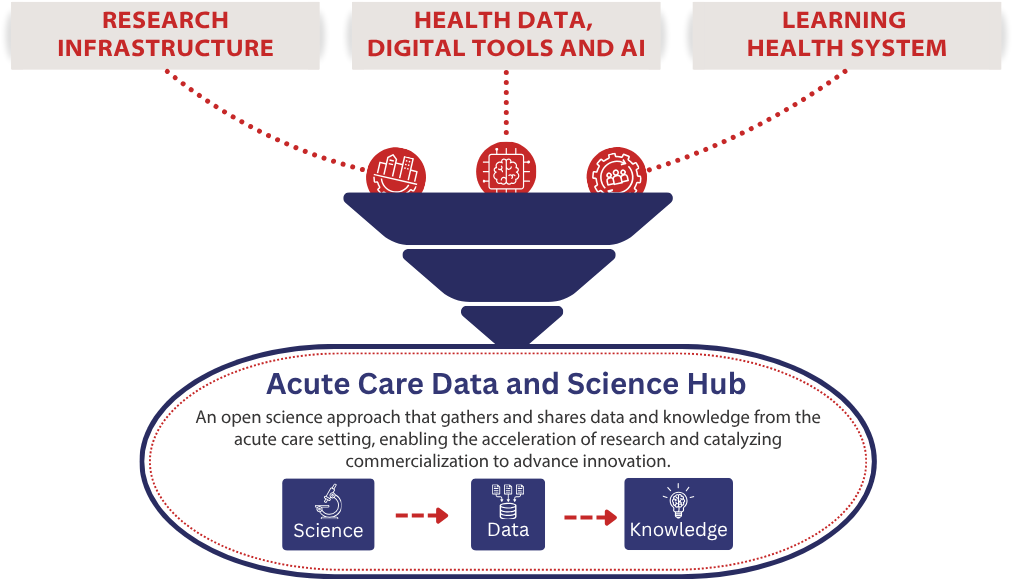
Acute Care Data and Science Hub
An open science approach that gathers and shares data and knowledge from the acute care setting, enabling the acceleration of research and catalyzing commercialization to advance innovation.
Long description
The graphic is a funnel-shaped diagram illustrating the flow of strategic enablers into an Acute Care Data and Science Hub. At the top of the funnel are three red icons:
- Research Infrastructure
- Health Data, Digital Tools and AI
- Learning Health System
These elements flow downward into the central section labeled "Acute Care Data and Science Hub". Beneath this label is a description that reads:
"An open science approach that gathers and shares data and knowledge from the acute care setting, enabling the acceleration of research and catalyzing commercialization to advance innovation."
At the bottom are three blue icons that are connected by arrows going from left to right, labeled:
- Science
- Data
- Knowledge
Research Infrastructure
ICRH will work to strengthen the platforms and tools across all research pillars required for cutting-edge research, including multi-disciplinary networks across disease pools, clinical trial networks, biobanks, and data-sharing protocols. We will advocate for pan-Canadian interdisciplinary networks and shared infrastructure to support scalable innovation and we will engage with CIHR and federal partners to align funding priorities with health system and policy.
We aim to modernize the biomedical and clinical trial ecosystem by increasing capacity across small and large institutions, facilitating approvals and ethics reviews and expanding access to clinical trial training. As Canadian jurisdictions step up efforts to attract new clinical trials in Canada, ICRH will work with its research community and partners to expand opportunities and support for multi-institutional trials in its mandate areas.
ICRH supports research infrastructure and methodology across CIHR's research pillars:
- Biomedical Research
Focuses on understanding how every part of the human body works, right down to our cells. - Clinical Research
Helps discover safer, smarter ways to prevent, diagnose, and treat diseases, with the help of volunteer participants. - Health Services Research
Focuses on improving healthcare for everyone. - Social, Cultural, Environmental and Population Health Research
Aims to improve the health of entire communities.
Health Data, Digital Tools and AI
Canada's health data ecosystem is undergoing a profound transformation, driven by technological advances that enable new ways to collect, analyze, share and act on health information. Realizing this potential requires strengthening the core infrastructure, including expanding access to multi-dimensional data, enabling responsible data sharing, and ensuring ethical governance. These pillars, aligned with the Pan-Canadian AI for Health (AI4H) Guiding Principles and the Pan-Canadian Health Data Charter, are essential to drive innovation, advance science and embed evidence-based solutions and informed decision-making into health systems where they make the greatest impact.
Building on the Joint Action Plan on Health Data and Digital Health [ PDF (2.2 MB) - external link ] and the Pan-Canadian Health Data Strategy, ICRH will advocate for a more connected, agile and data-driven health ecosystem, standardized ethical data collection and sharing, enhanced interoperability across jurisdictions and aligned principles of data stewardship and indigenous data sovereignty. To harness these innovations and remain at the forefront of a digitally enabled, AI-powered future, utilization of AI and digital health technologies will be encouraged to optimize study design, research conduct and accelerate discovery to support clinical decision-making, diagnosis, monitoring and treatment.
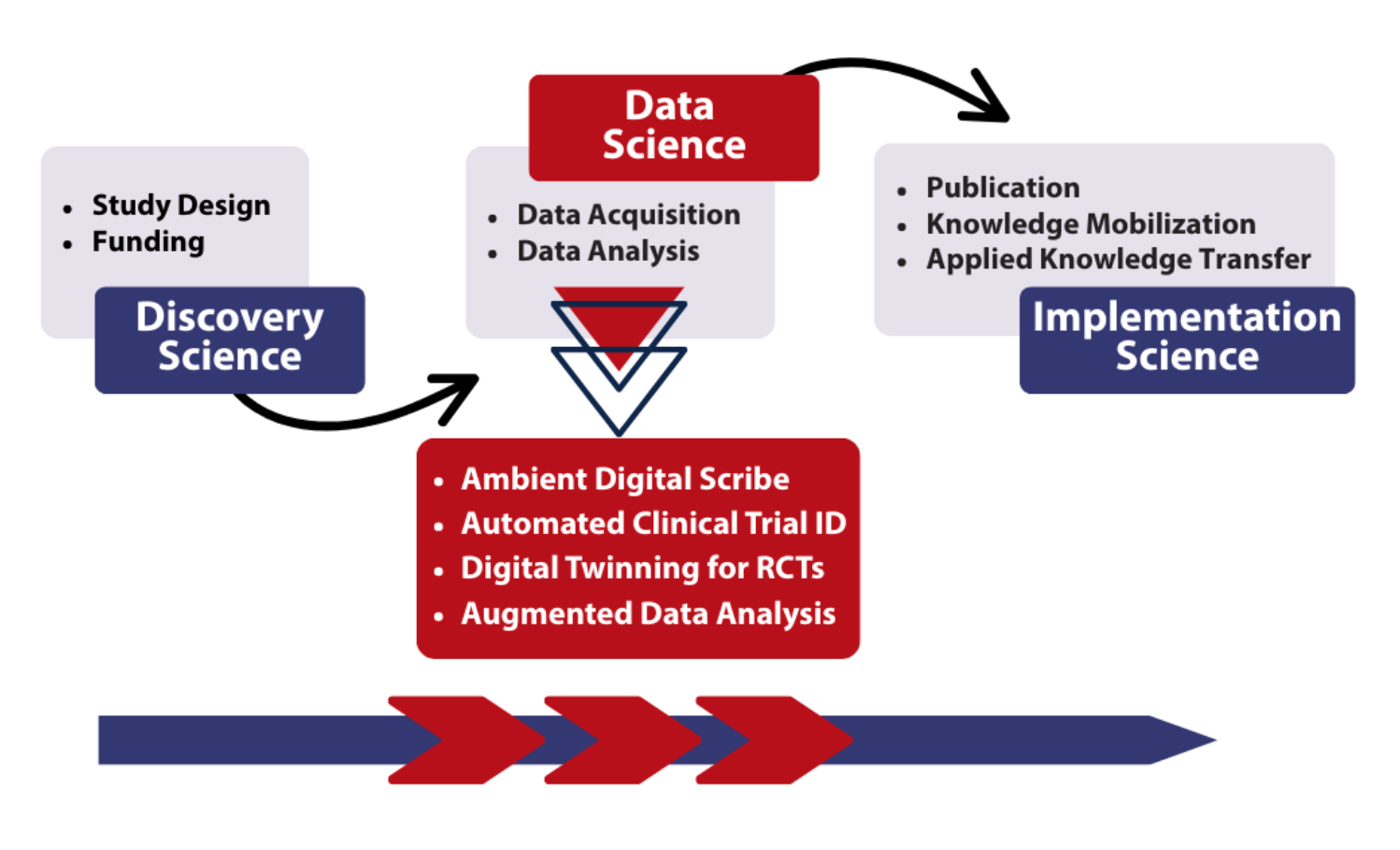
The figure below illustrates how AI integration can accelerate the entire research-to-impact pipeline, from discovery through data acquisition and analysis to real-world implementation. Emerging tools such as ambient digital scribes, automated trial matching, digital twinning for randomized clinical trials (RCTs) and AI-augmented analytics represent some of the most promising technologies driving this transformation. These tools will help streamline implementation by facilitating publication, knowledge mobilization, and applied knowledge transfer.
Reducing Gestation Time from Discovery Science to Implementation Science
Long description
This graphic represents a flow chart to show how data science can reduce the gestation time from discovery science to data science to implementation science.
- Discovery Science includes:
- Study Design
- Funding
- Data Science includes:
- Data Acquisition
- Data Analysis
- Implementation Science includes:
- Publication
- Knowledge Mobilization
- Applied Knowledge Transfer
Beneath the data science section, a red-highlighted area lists advanced digital tools and methods:
- Ambient Digital Scribe
- Automated Clinical Trial ID
- Digital Twinning for RCTs
- Augmented Data Analysis
Underneath this list, (3) three red arrows represent the potential acceleration of this research phase that could be provided by digital tools and methods.
Learning Health System
ICRH envisions a future where research is brought to the forefront of healthcare settings, contributing to better care and informed decision-making.
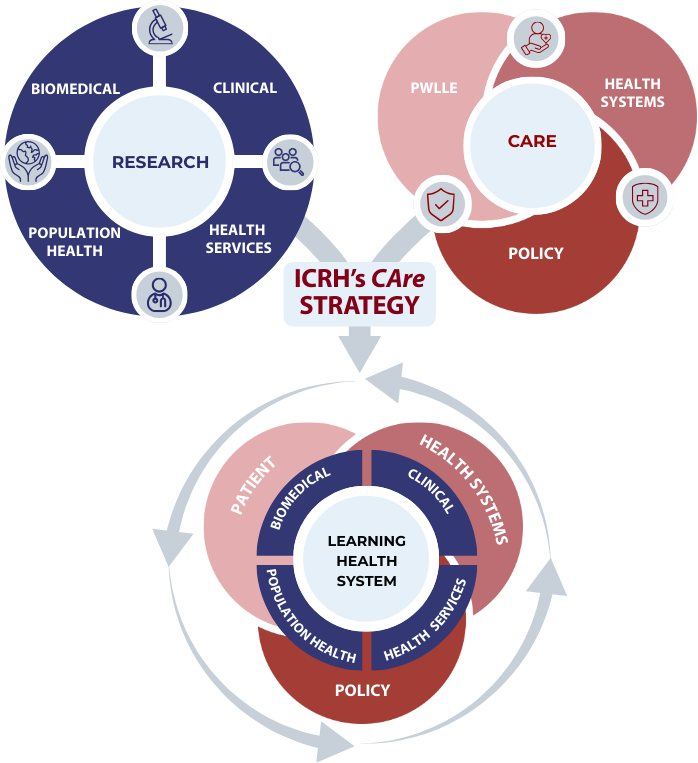
Rooted in CIHR's research pillars (biomedical, clinical, health services, and population health), ICRH's CAre strategy proposes to bridge the gap between research and key care components within a Learning Health System framework.
ICRH aspires to support a dynamic learning health system in which research serves as the foundation, integrating meaningful engagement with People with Lived and Living Experience (PWLLE), and embedding patient and health systems' data and knowledge. By actively engaging policymakers and decision-makers, this concept will drive sustainable, evidence-based improvements across the continuum of care.
Long description
The diagram illustrates how research and care domains can converge to form a Learning Health System as part of our CAre Strategy. It is composed of three main interconnected sections:
- Research (Top Left: Blue Circle)
- This blue circle is divided into four quadrants, each representing a distinct pillar of health research:
- Biomedical
- Clinical
- Population Health
- Health Services
- This blue circle is divided into four quadrants, each representing a distinct pillar of health research:
- Care (Top Right: Red Circle)
- The Care section is represented with three smaller red circles branching out and forming a unified circle. Each smaller circle signifies a key influencer in healthcare:
- PWLLE (People with Lived and Living Experience)
- Health Systems
- Policy
- The Care section is represented with three smaller red circles branching out and forming a unified circle. Each smaller circle signifies a key influencer in healthcare:
- Learning Health System (Bottom: Merged Blue and Red Circle)
- At the bottom of the diagram is a larger circle, visually blending the blue and red elements from the top sections.
- The inner blue layer features the research pillars: Biomedical, Clinical, Population Health, and Health Services
- Surrounding this, an outer red layer includes care influencers: PWLLE, Health Systems, and Policy
- At the bottom of the diagram is a larger circle, visually blending the blue and red elements from the top sections.
Arrows and Flow Representation
- A two-headed arrow connects the Research (blue circle) and Care (red circle) sections at the top of the diagram, and funnels downward through the central box labeled ICRH's CAre Strategy. From the central box, the arrow continues downward into the Learning Health System circle at the bottom. Surrounding the Learning Health System circle, a circular flow arrow wraps around the entire section.
Strategic Implementation
ICRH's CAre strategy will unfold through three phases designed to strengthen the research ecosystem, expand collaborative capacity and deliver measurable results in acute care.
Phase 1: 2024-2025
Foundational Phase: Harnessing our Foundation
This first phase is leveraging established and emerging teams in key areas to foster multidisciplinary collaborations and national research networks. These initiatives strengthen mechanisms for equity, patient engagement, and capacity-building to support a more inclusive, sustainable future. Team grants launched up to 2025 set the conditions for broader systemic transformation.
Phase 2: 2025-2028
Strengthening Phase: Unifying for Impact
Currently underway, this phase focuses on cross-sector alignment. ICRH is pursuing key research priorities alongside strategic themes. ICRH is actively partnering with other CIHR Institutes to amplify impact by supporting key complementary initiatives and committing to cross-cutting innovation, aligned with national priorities. These initiatives underscore ICRH's engaged collaborations and shared leadership toward interdisciplinary research and real-world evidence implementation.
Phase 3: 2027-2034
Coalition Phase: Catalyzing the Future
Looking ahead, ICRH will launch a coalition-based initiative to drive national transformation in acute care delivery. This final phase envisions co-investment by funders, innovators, provinces, and academic leaders in translational accelerators, predictive care models, and recovery science. The aim is to drive whole-system improvement, reducing preventable hospitalizations, improving discharge outcomes, and positioning Canadian science as a global benchmark for acute care excellence.
Strategic Investments
ICRH holds a unique position within Canada's health research ecosystem, as a bridge between discovery and implementation science, between researchers and policymakers and between community needs and national strategies. Our role is more than funding research; it's shaping the direction of research in our mandate areas, building alliances, and amplifying its impact.
ICRH will leverage its traditional and emerging assets to build support and capacity to achieve its objectives. Capacity building will centre around emerging innovator scientists and computational clinicians. These assets are organized around the following themes:
- Knowledge Mobilization: Connect researchers, policymakers, and communities to translate research into actionable policy and practice.
- Pan-Canadian Networks: Co-design interdisciplinary initiatives within the federal research ecosystem, health charities, industry and community to break down silos and amplify impact.
- Capacity Building: Provide targeted funding, awards and salary mechanisms for trainees, early career researchers, clinician and basic scientists to foster innovative approaches to training.
- Research Infrastructure: Expand health data and clinical trial platforms and champion shared stewardship for biobanks and registries to accelerate research.
- Equity in Research: Engage Indigenous communities and equity-deserving groups in research activities, ensuring co-design and early involvement in decision-making.
- Policy: Strengthen relationships with key government partners across all levels to align research with policy priorities and facilitate the translation of research evidence into new policies.
Strategic Partnerships
Partnerships are a backbone of ICRH's CAre strategy and a key lever for achieving both scientific and system-level impact.
Aligned with the federal government's vision to grow Canada's innovation economy, ICRH will develop a tailored partnership strategy aligned with ICRH CAre vision and framework. We will identify, assess, prioritize, and steward strategic collaboration for impact across internal and external sectors, building a targeted, high-value partnership framework that connects prospective and existing partners with ICRH's priorities. With this focused, selective and principled approach, ICRH aims to position itself as the partner of choice in Canada's circulatory and respiratory research landscape.
Engagement and Partnership
The incidence and outcomes of cardiovascular and respiratory diseases are profoundly influenced by social and structural determinants of health. To advance equitable health outcomes, our research must be rooted in understanding these determinants and their intersections with biological factors. Our partnerships and engagements will be built on mutual respect, cultural awareness, and shared goals, with the aim of developing impactful, community-informed solutions.
Indigenous Communities
Guided by our shared commitment with CIHR to "Accelerate the Self-Determination of Indigenous Peoples in Health Research", ICRH's partnership strategy will prioritize respectful, sustained engagement with Indigenous communities to ensure meaningful representation across our research activities. We will also partner with Indigenous organizations, scholars and communities to co-develop initiatives that respond to emerging health challenges within our mandate areas, such as inequitable access to care and the disproportionate burden of chronic diseases. To further build capacity in Indigenous health research, ICRH seeks to leverage existing Indigenous-led networks and platforms, such as the Network Environments of Indigenous Health Research (NEIHR).
Equity-Deserving Communities
In parallel, ICRH is committed to engaging with underrepresented and equity-deserving groups to foster inclusive participation and ensure our research reflects the diverse lived experiences of groups facing systemic barriers to health.
Internal Partnership Strategy
ICRH will strengthen collaboration within CIHR by working in areas of aligned interest with peer institutes and co-developing joint and synergistic initiatives that reflect shared priorities. This approach supports the CIHR 2021-2031 Strategic Plan, which emphasizes inclusive research excellence, reconciliation in health research, meaningful health system impact, and evidence-informed decision-making.
Positioned along the research continuum, from bench to bedside, ICRH will continue to contribute to CIHR established initiatives and programs (SPOR, NEIHR, REDI, etc.). Moreover, we will explore the possibility of partnering with other funding agencies that are part of the federal research ecosystem, like the Natural Sciences and Engineering Research Council of Canada (NSERC) and the Social Sciences and Humanities Research Council of Canada (SSHRC) to foster interdisciplinary research opportunities.
External Partnership Strategy
ICRH will actively seek out external partnerships that fuel homegrown innovation. This includes working with pan-Canadian health organizations to pursue implementation-focused coalitions with provincial ministries, hospital networks, and public/private-sector partners to ensure that research translates into solutions that are scalable, practical, and responsive to needs across the country. ICRH will also re-engage long-standing allies and develop new relationships with health charity organizations to strengthen and diversify its collective impact. We are interested in partnerships to accelerate clinical trials, scale AI platforms, and ensure economic benefits of research for Canadians. Our aim is to harness venture philanthropy to position ICRH-supported science as a catalyst for national health resilience and economic renewal. ICRH aims to co-create catalyst showcase events to facilitate the convergence of scientific innovation and industry investment, fostering partnerships that translate ideas into impact.
Conclusion: Reimagining Acute Care Together
Canada stands at a pivotal moment. Pressures on our health systems are growing, but so too is our capacity to respond with bold science, smart policy, and transformative collaboration. ICRH is stepping forward with a clear plan to lead this response, backed by a renewed commitment to impact, equity, and innovation.
Just as our predecessors once cooled the human body to repair the heart motivated by need, committed to sound science, and unafraid to try, so too is ICRH rising to today's challenge. The same spirit that once pioneered open-heart surgery and life-saving interventions now fuels a new era of research-driven science and transformation.
This opportunity is timely. The IRPP is more than a roadmap, it is a catalyst. It aligns with CIHR's strategic vision and reflects the federal government's national agenda to mobilize science and innovation for inclusive growth and public good. It positions ICRH as a key driver of health system renewal, economic opportunity and better outcomes for people of all ages across Canada.
We invite our colleagues, partners, and leaders across all sectors to join us. The stakes are high, but the possibilities are even higher. Together, we can close the gap between knowledge and action, ensuring that every discovery finds its way to the people and systems that need it most.
Acknowledgements
The Institute of Circulatory and Respiratory Health (ICRH) extends its sincere appreciation to everyone who contributed to the development of our 2024-2034 Institute Research Priority Plan (IRPP). We are deeply grateful to the members of our diverse research community who have generously contributed their time, expertise and lived experiences throughout our research priority-setting process.
We gratefully acknowledge the collaboration and support of our CIHR and Institute colleagues, including our Institute Integrated Team (IIT).
We also thank the ICRH Institute Advisory Board (IAB) for their ongoing guidance and leadership as well as the MP Advisory Group (MPAG) for their dedicated involvement at every stage of the IRPP process.
Together, your collective wisdom has helped define a bold and inclusive vision for the future of circulatory and respiratory health research in Canada and beyond.
Institute Staff
- Associate Director
Marie-Claude Gingras, PhD - Assistant Scientific Director
Annina Spilker, PhD - Lead, Science Programming
Niobe Haitas, PhD - Lead, Analytics
Suomiao Xing, MScPH - Lead, Communications
Emanuelle Bernard-Bédard - Lead, Administrative Services & Operations
Veronica Atehortua - Co-Lead, Event Planning
Juliana Veleno - Co-Lead, Finance
Sara Lafond, MSc
IAB Members
- Mireille Ouimet (Chair)
Scientist, Director, Cardiovascular Metabolism and Cell Biology Laboratory, University of Ottawa Heart Institute
Associate Professor, Department of Biochemistry, Microbiology and Immunology, Faculty of Medicine, University of Ottawa - Dennis T. Ko (Vice-Chair)
Professor, Department of Medicine, University of Toronto
Senior Scientist, Sunnybrook Research Institute
Senior Scientist, ICES
Interventional Cardiologist, Schulich Heart Centre, Sunnybrook Hospital - Shawn Aaron
Professor, Department of Medicine, University of Ottawa
Senior Scientist, Ottawa Hospital Research Institute - Kerstin de Wit
Professor, Department of Emergency Medicine
Queen's University, Kingston, Ontario - Charles Tam
Director of Regulatory Affairs & member of Canadian Leadership Team, Edwards Lifesciences - Indra Narang
Professor of Paediatrics, University of Toronto
Senior Scientist, SickKids Research Institute
Associate Chair, Faculty Development, Equity, Diversity and Inclusion, Hospital for Sick Children - Kara Patterson
Physiotherapist, Associate Professor, Department of Physical Therapy, University of Toronto
Senior Scientist, KITE-Toronto Rehabilitation Research Institute
Lead, RELEARN Lab - Nishita Singh
Stroke Neurologist
Assistant Professor, Neurology, University of Manitoba
Clinical Stroke Research Chair, Heart & Stroke & Research Manitoba - Alexandra King
Cameco Chair, Indigenous Health and Wellness, University of Saskatchewan - Patrice Lindsay
Health Systems and Engagement Consultant, MarcLind Health Systems Consulting - Jason Acker
Senior Scientist, Canadian Blood Services
Professor, Department of Laboratory Medicine and Pathology, University of Alberta - Ejaife Agbani
Assistant Professor, Physiology and Pharmacology, University of Calgary - Sudi Barre
Edmonton, Alberta
Patient with Lived Experience, Wellness Coach
- Date modified: